
The Importance of Hydration In Healing
Summary: Living in the Middle East has heightened my appreciation for water’s essential role in health. For Type 1 diabetes, maintaining hydration is critical during both daily life and illness to manage blood sugar levels. Monitoring urine colour and using apps like ‘My Water Balance’ help ensure adequate intake, supporting overall well-being and hydration goals.
Since arriving in the Middle East, I have become so much more mindful of the importance of water in my daily life. It is a precious commodity out here, one that you do not want to be without. The few days of rain that happen are greeted with a sense of wonder and even the occasional moment of celebration or joy.
Hydration For Type 1 Diabetes During Illness
Somewhere in the back of my mind, I guess I’ve always known that there is a connection between T1D and hydration. After all, I can still recall those feelings as a kid of severe thirst that accompanied a way-too-high blood sugar – whether due to illness or any other one of an unending list of factors that randomly caused my blood sugars to spike! I recall that feeling of believing that, no matter how many cups of water I drank, it would never be enough. It felt like my thirst would never again be quenched.
Hydration In Daily Life
Okay, so we pretty much all understand that hydration during illness is a biggie for us diabetic types. But what about the other (hopefully) 99% of our lives, when we’re just tootling about in our days in normal (perfect?!) health…? Is it important then?
For type 1 diabetes, hydration is even more important. In fact, dehydration has been found to favour the development of hyperglycaemia (high blood sugars) in diabetes. I searched around for more information on why that might be the case. Whilst I couldn’t find anything directly related to type 1 diabetes, I did come across an interesting study that investigated the relationship between water intake and blood glucose regulation in type 2 diabetics.
How Much Water Is Enough Water?
Taking that 8 cups of water as a baseline, there are still certain factors that cause this quantity to be revised for any given individual. These factors include:
| Variable | Exemplar Research Findings | |||||||
|---|---|---|---|---|---|---|---|---|
|
Gender |
The average woman requires 2.7 litres of water per day, whilst the average man requires 3.7 litres. [1] |
|||||||
|
Age |
Elderly people who drink 8 glasses of fluid per day may actually be overhydrated. [2] |
|||||||
|
Socioeconomic Status |
Water intake is lower in lower-income adults and those with lower education. [3] |
|||||||
|
Environment |
Hot climates, such as those found in desert environments, cause increased fluid loss due to sweating. [4] |
|||||||
|
Exercise |
Strenuous exercise can cause sweat rates up to 2-3 litres per hour. [5] |
|||||||
|
Medical Conditions |
Excess hydration should be avoided for people with cardiovascular disorders, pronounced chronic renal failure and endocrinopathies, amongst other medical disorders. [6] |
|||||||
So I think that this shows how most, if not all, people are likely to not need the ‘standard’ amount of recommended water intake! So how can I, or anyone else, work out how much their particular body, with its own particular nuances, needs to stay healthy? Thankfully, our bodies have their own built-in alert system…
The Human Body’s ‘Hydration Alert System’… Thirst And Urination!
Our bodies have all the expertise they already need, just packed away inside them. All we have to do is listen and pay attention!
So, hydration… The first and obvious sign of lacking sufficient water is that you will become thirsty. This is your cue to drink. So do so! Unfortunately, in today’s world, the thirst system in the human body can go offline. If you have ignored your body’s cries for water a few too many (thousand!) times, then your body is likely to save its cries for the most extreme times, when hydration is a must. Therefore, if this might be the case for you, check your urine… What colour is it?
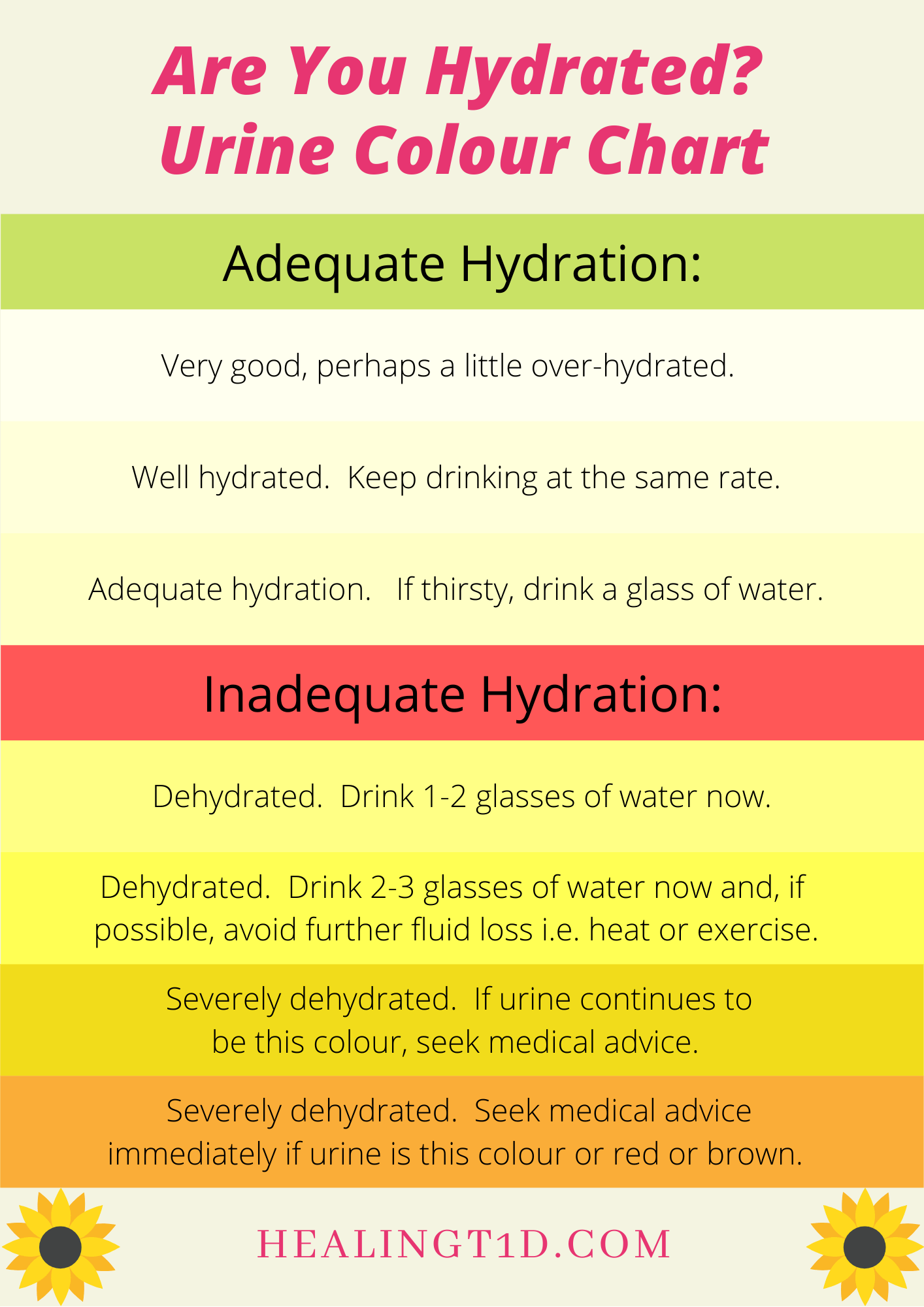
If your urine is anything darker than a light summer lemonade, then you are dehydrated (or, if very dark, you could have another medical issue going on and you should go to your doctor pronto!). Each time you urinate, check the colour. In an ideal world, you would check your colour by taking a sample in a suitable collecting container that only has the urine sample in it. However, as most of us probably go to the toilet in the, yep, toilet(!) with the water already in the toilet bowl, we’ll just have to use that as a best guess effort. But, bear in mind, if the urine in the toilet bowl is darker than it should be, then you are definitely dehydrated and need to take action soonest.
Generally, if you have a pale straw-like colour of urine, drink frequently and rarely feel thirsty, then you’re on the right track. I, on the other hand, know that I have some work to do on this! Now where did I leave my water bottle…??
Improving Water Intake
In trying to improve water intake, there are a couple of things that have worked for me. First of all, I have found an app called ‘My Water Balance-Intake Drink’ by Viktor Sharov. It has a nice reminder feature that gently nags (reminds?!) me through the day to take another sip. I like that it shows me what percentage of my water has been drunk whenever I input a drink so that I feel that I’m making progress each day.
I also have a gentle reminder about water consumption every time I visit the ladies’ room! If my urine isn’t clear in the toilet bowl, it automatically reminds me to go and get another drink.
The other thing that has really helped me is creating habits around fluid intake. First thing in the morning, I go downstairs to get a litre bottle of water. That comes with me into my meditation space and I sip on it during that first hour of my day that I devote to my spiritual practices. Having already had 1 litre by the time I finish that hour, I already feel confident about completely my water intake for the day. I also have the habit to sit down with a glass of water with every meal. I understand that drinking water half an hour before a meal helps with digestion and not overeating but that habit’s never stuck with me so I go for the ‘glass with a meal’ approach instead – it’s better than not having any!
How do you track your fluids? What do you do to encourage yourself to hydrate more? I’d love to hear and learn from your ideas too!


References:
2. Picetti, D., et al. (2017). Hydration health literacy in the elderly. Nutrition and Healthy Aging, 4(3), 227-237. [Link]
3. Rosinger, A. Y., et al. (2018). Disparities in plain, tap and bottled water consumption among US adults: National Health and Nutrition Examination Survey (NHANES) 2007-2014. Public Health Nutrition, 21(8), 1455-1464. [Link]
4. Sawka, M. N., et al. (1998). Hydration Effects on Temperature Regulation. International Journal of Sports Medicine, 19, S108 – S110. [Link]
5. Shirreffs, S. M. (2009). Hydration in sport and exercise: water, sports drinks and other drinks. Nutrition Bulletin, 34(4), 374-379. [Link]
6. Manz, F. (2007). Hydration and Disease. Journal of the American College of Nutrition, 26(5), 535S-541S. [Link]

GET HEALINGT1D’S FUTURE ARTICLES IN YOUR INBOX!
Get the latest musings and findings straight to your email inbox.

Natalie is a blogger with Type 1 Diabetes. Natalie’s special gifts are questioning the status quo and being a rebel. She is using these gifts to question medical ‘knowledge’ and find a true cure for Type 1 Diabetes.































Recent Comments: